Advice to the Profession: End-of-Life Care

Last Updated: March 2023
Advice to the Profession companion documents are intended to provide physicians and physician assistants ("Registrants") with additional information and general advice in order to support their understanding and implementation of the expectations set out in policies. They may also identify some additional best practices regarding specific practice issues.
This document provides guidance on how the obligations set out in the Decision-Making for End-of-Life Care policy can be effectively discharged. This document also provides physicians with guidance on other specific end-of-life care issues, such as medical certificates of death and dying at home.
Advance Care Planning and Goals of Care Discussions
What are the differences between advance care planning and goals of care discussions? If I have these discussions, do I still need to obtain consent for treatment?
The main difference between advance care planning and goals of care discussions is the context of the decision-making: where advance care planning discussions take place earlier and help prepare patients and their substitute decision-makers for future decision-making, goals of care discussions occur in the context of a significant illness or disease when there are treatment or care decisions that will need to be made in the near future, and help inform which treatment options may be provided.
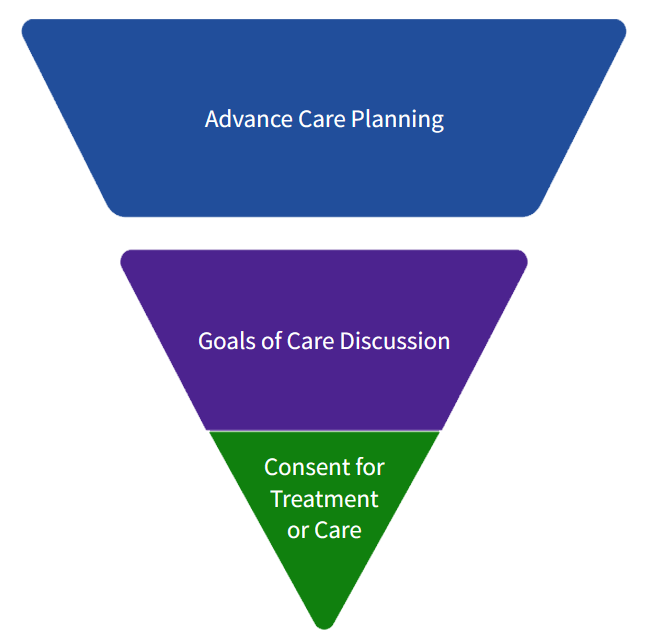
As illustrated in the diagram below from Hospice Palliative Care Ontario, neither advance care planning nor goals of care discussions constitute consent. An advance care planning discussion may outline information about the prior capable wishes of a patient and may be used to guide substitute decision-makers in providing informed consent, but it does not constitute consent to treatment. Similarly, a goals of care discussion will often lead to the proposal of treatment options and/or the development of a plan of treatment, but it does not constitute consent to treatment. Accordingly, even if you have these discussions, you will need to obtain consent from your patient or their substitute decision-maker in order to provide treatment.
 | Advance Care Planning
Goals of Care Discussion
Consent for Treatment or Care
|
What are the benefits of having timely advance care planning and goals of care discussions? What resources can I use or direct my patients to?
Having timely end-of-life care discussions can, among other things:
- lead to improved patient outcomes and quality of life;
- inform treatment decisions and ensure that the care provided aligns with the patient’s wishes, as well as their personal, cultural and religious/spiritual values and beliefs;
- lessen family distress;
- increase patient comfort with physicians making decisions to write orders to withhold resuscitative measures;
- decrease potentially harmful or overly aggressive interventions and treatments;
- encourage realistic treatment goals; and
- help ensure the health-care team is not rushing to have last-minute conversations during an emergency, for example, when a patient is experiencing a cardiac or respiratory arrest.
It is important for physicians to take an active role in helping patients and/or substitute decision-makers identify meaningful and realistic goals of care that seek to incorporate the patient’s – not the substitute decision-maker’s – wishes, values, and beliefs. Patients and/or substitute decision-makers may need some assistance articulating these wishes, and physicians can help them engage in this process by providing necessary medical information and opportunity for discussion.
The following websites may be helpful:
- Advance Care Planning Canada has resources and tools to assist both physicians and patients in making decisions regarding end-of-life care.
- Advance Care Planning Ontario and Dying with Dignity Canada both offer advance care planning workbooks tailored to patients receiving care in Ontario.
- Choosing Wisely Canada also has resources to help both physicians and patients get started in having end-of-life discussions.
- Hospice Palliative Care Ontario also sets out information for physicians about advance care planning and goals of care
When should I be initiating discussions about advance care planning?
Where a patient’s specific circumstances and health status would make it appropriate to initiate a discussion about advanced care planning, physicians who provide care as part of a sustained physician-patient relationship are required, where possible, to do so. That said, it is never too early for physicians to have discussions about advance care planning with their patients. As part of routine care, physicians may discuss the importance and benefits of advance care planning; choosing a substitute decision-maker; documenting and disseminating advance care plans to substitute decision-makers and health-care providers; and reviewing these plans periodically throughout life.
When significant life events or changes in the patient’s medical status occur, physicians can also remind patients of the importance of advance care planning and encourage patients who have already engaged in the process to evaluate existing care plans.
When should I be initiating goals of care discussions?
The policy requires physicians, where possible, to initiate goals of care discussions with patients who have a significant illness or disease and are at risk of clinical deterioration in the foreseeable future.
The policy recognizes that there are limits to when physicians will be able to initiate goals of care discussions. For example, it may not be possible to have these discussions when a patient is acutely deteriorating. It is situations like this that underscore the importance of having these discussions as early as possible.
Why might it be important to involve family members and/or others close to the patient in discussions about the patient’s care?
Family and/or others close to the patient can act as intermediaries; ask clarifying questions; and help patients to better understand their diagnoses, prognoses, medications, any tests that may be required, as well as the decisions they have to make about treatment options. Involving family and/or others close to the patient in ongoing care can also result in patients receiving more effective care and support at home and can mitigate caregiver distress.
It is important to ensure that consent is obtained to disclose personal health information whenever a patient and/or substitute decision-maker wishes to involve others in the patient’s care.
Should I be documenting advance care planning and goals of care discussions?
Yes. In keeping with the College’s Medical Records Documentation policy, physicians must document every encounter with a patient and/or substitute decision-maker and all patient-related information. In the end-of-life context, this means that physicians must document references to discussions and decisions regarding treatment, goals of care, and advance care planning, and explicitly and clearly reference when an order to withhold resuscitative measures has been placed in the patient’s record.
Life-Sustaining Treatment
Can I offer life-sustaining treatment to patients on a trial basis? How would that work?
Yes. There are times where the outcomes of life-sustaining treatment are uncertain, and in these instances, proposing a trial of treatment allows for the exploration of a possibly positive outcome.
When offering a trial of treatment, it is important to explain to the patient and/or substitute decision-maker which outcomes would warrant continuation and discontinuation of the treatment. It is also important to explain that when the patient and/or substitute decision-maker provide consent to the trial of treatment, they may at the same time provide consent to discontinue the treatment at a later stage if it proves ineffective. Providing consent to discontinue the treatment up front is helpful because it eliminates the need to formally get consent from the patient and/or substitute decision-maker to stop the trial of treatment down the road.
Once the treatment has been initiated, patients and/or substitute decision-makers can withdraw their consent to any elements of the trial and/or withdraw their consent to discontinue the treatment at any time, and it is important to communicate this to the patient and/or substitute decision-maker. When consent to discontinue the treatment is withdrawn, any disagreement with the physician about continuing the treatment would be managed in accordance with the policy provisions on withdrawing potentially life-sustaining treatment.
What is the role of the Consent and Capacity Board? How do I find more information?
The Supreme Court of Canada has affirmed that the Consent and Capacity Board (CCB) is the appropriate authority to adjudicate disagreements between physicians and substitute decision-makers regarding the withdrawal of life-sustaining treatments. The CCB is an expert tribunal, comprised of lawyers, psychiatrists, and members of the public, and is supported by full-time legal counsel. The CCB has the ability to convene hearings quickly and has the authority to direct substitute decision-makers to make decisions in accordance with a patient’s prior capable wishes or best interests.
The CCB can also provide assistance when a physician believes that a substitute decision-maker is not acting in the best interests of a patient, or when clarity is required to determine a patient’s wishes, whether a wish applies, or whether a wish was expressed while the patient was capable or at least 16 years of age. The CCB can also grant permission to depart from wishes in very limited circumstances.
The CCB’s website has information regarding their services. Physicians may wish to contact the CCB directly for more assistance or seek assistance from legal counsel, either from their institution, if applicable, or from the Canadian Medical Protective Association.
Withholding Resuscitative Measures
What are the legal requirements regarding withholding resuscitative measures?
In August 2019, the Ontario Superior Court released Wawrzyniak v Livingstone, which clarified that physicians are required to provide cardiopulmonary resuscitation (CPR) to a patient only when doing so is within the standard of care.
Where a physician determines that it is not appropriate to provide resuscitative measures, such as CPR, to a patient (i.e., that it is not within the standard of care), the physician is not required to obtain consent from the patient and/or substitute decision-maker prior to withholding resuscitative measures and/or writing a Do Not Resuscitate order (referred to in the Decision-Making for End-of-Life Care policy as an “order to withhold resuscitative measures”).
Does the College require physicians to obtain consent before writing an order to withhold resuscitative measures?
No, in keeping with the court’s decision in Wawrzyniak v Livingstone (Wawrzyniak), the College does not require physicians to obtain consent from a patient and/or substitute decision-maker prior to writing an order to withhold resuscitative measures. However, physicians have other professional obligations they must meet when writing these orders.
When the risk of harm in providing resuscitative measures to a patient outweighs the potential benefits
There are times where it may be possible to resuscitate a patient, but the physician determines that the risk of harm in providing resuscitative measures outweighs the potential benefits. This risk-benefit calculation involves subjective value judgments. As a result, before making these determinations, the policy requires physicians to consider the patient’s wishes, as well as the patient’s personal, cultural and religious/spiritual values and beliefs, if they can be ascertained and/or the physician is aware of them. In order to respect the importance of these decisions for patients/families, the policy also requires physicians to do several things before writing an order to withhold resuscitative measures:
- inform the patient and/or substitute decision-maker that the order will be written;
- explain to the patient and/or substitute decision-maker why resuscitative measures are not appropriate, including the risk of harm in providing resuscitative measures and the likely clinical outcomes if the patient is resuscitated; and
- provide details to the patient and/or substitute decision-maker regarding clinically appropriate care or treatment(s) they propose to provide.
It is also helpful for physicians to re-articulate the patient’s wishes, values, and beliefs when informing the patient and/or substitute decision-maker that an order to withhold resuscitative measures will be written. This can help reassure the patient and/or substitute decision-maker that the physician has understood the patient’s wishes, values, and beliefs.
Recognizing that decisions need to be made quickly when a patient’s condition deteriorates rapidly, the policy permits physicians to write an order to withhold resuscitative measures in the patient’s record and subsequently comply with the expectations set out above where there is an imminent need to write an order. While the policy still requires physicians to consider the patient’s wishes, values, and beliefs in these emergent situations, physicians do not have to discuss them with the patient and/or substitution decision-maker if there is no time to do so. However, if the physician is already aware of the patient’s wishes, values, and beliefs, they are required to factor them into their decision-making.
When might a physician determine that the risk of harm in providing resuscitative measures to a patient outweighs the potential benefits?
A patient’s medical condition may be such that providing resuscitative measures would cause more harm than good, and would possibly not successfully resuscitate the patient. For example:
- An adult with septic shock who is non-responsive to optimal intensive care develops multiorgan failure.
- An older adult with progressive pulmonary hypertension and right heart failure presents with acute bronchopneumonia and secondary cardiovascular collapse.
- An adult with stage III pancreatic cancer presents with ascites secondary to peritoneal metastases.
- An older, non-verbal adult with progressive dementia who refuses to eat or drink on their own presents to hospital with fever and pyuria. There is a history of recurrent urinary tract infection secondary to multidrug-resistant organisms.
- An anencephalic infant with preserved brainstem function but no higher cognitive abilities initially requires mechanical ventilation. Although initially able to be weaned from the ventilator, the infant suffers ongoing respiratory distress requiring repeated hospital admissions for ventilatory support.
Determining whether the risk of harm in providing resuscitative measures to a patient would outweigh the potential benefits in these scenarios involves considering the patient’s medical condition, as well as their wishes, values, and beliefs, if they can be ascertained, and then assessing whether, among other things:
- the potential outcome would constitute a success for the patient (e.g., whether success means survival, discharge from intensive care, or discharge from hospital);
- the probability of success is sufficiently high to warrant providing resuscitative measures in light of the risk of harm; and/or
- the patient’s quality of life would be tolerable to them if they survived.
Physicians will need to use their professional judgment on a case-by-case basis to determine whether the risk of harm in providing resuscitative measures to a patient would outweigh the potential benefits. When feasible, it can be helpful for physicians to make these decisions in discussion with other health-care providers. It is also important that physicians consider how their own values, beliefs, and implicit biases may affect their assessment of whether the risk of harm in providing resuscitative measures to a patient would outweigh the potential benefits. As outlined above, this risk-benefit calculation involves considering matters from the patient’s point of view as much as possible.
How can I explain to a patient and/or substitute decision-maker why resuscitative measures are not being offered?
It may be helpful to explain that just as patients would not be offered a surgery or other treatment that is not within the standard of care, patients are not provided resuscitative measures that are not within the standard of care.
The policy requires physicians to inform/reassure the patient and/or substitute decision-maker regarding clinically appropriate care or treatment(s) they propose to provide – what does this mean?
As outlined in the policy, physicians may determine that a patient’s condition is such that it is appropriate to either withdraw life-sustaining treatment or withhold resuscitative measures. However, it is critical for patients and/or substitute decision-makers to understand that even when that is the case, the patient will not be abandoned. Rather, the patient will continue to receive care or treatment that is clinically appropriate, such as palliative care, surgical procedures that are clinically indicated (e.g., fracture repair), and/or chronic disease management (e.g., diuretic therapy for heart failure).
What happens if there is disagreement about the writing of an order to withhold resuscitative measures?
Given that physicians are not required to obtain consent before writing an order to withhold resuscitative measures, they can write an order even if the patient and/or substitute decision-maker disagree. However, physicians must do several things to provide support to the patient and/or substitute decision-maker at the earliest opportunity after learning of a disagreement, as set out in the policy.
In addition, there are other things physicians can do to alleviate distress if a patient and/or substitute decision-maker expresses concern about the writing of an order to withhold resuscitative measures. For example, it is good practice to review the reasons for the order, where appropriate.
It is important to note that disagreements between the health-care team and patient/substitute decision-maker regarding orders to withhold resuscitative measures often relate to misunderstandings about what is involved in providing resuscitative measures, and/or stem from the concern that the order will result in neglect or very limited attention to otherwise treatable conditions unrelated to a cardiac or respiratory arrest. This is why it is important for physicians to review the reasons for the order, as noted above.
One of the types of resuscitative measures patients and/or substitute decision-makers might request is cardiopulmonary resuscitation (CPR). It is helpful to explain that CPR generally has a very low success rate – especially for frail patients, those who have a critical illness, and/or those with serious underlying medical conditions – and that the risks of CPR include harmful side effects and adverse clinical outcomes. If CPR is not successful, it may mean that the patient dies in an undignified and traumatic manner.
I want to have a conversation with my patient and/or their substitute decision-maker about the patient’s resuscitation code status – what should I be discussing?
Physicians can explain that full resuscitation is the default for all patients and that this means the health-care team will use any available resuscitative measure (e.g., chest compressions, artificial ventilation) to resuscitate a patient if the patient experiences a cardiac or respiratory arrest.
It can be helpful for physicians to have comprehensive discussions with patients and/or substitute decision-makers about what, if any, interventions the patient might want to receive. In some instances, patients may not want all elements of resuscitative measures and so it is important to explore this with patients and/or substitute decision-makers. It is good practice to explain that even if a patient and/or substitute decision-maker request full resuscitation, this request may be overridden in the future if a physician determines that it would not be appropriate to provide any or all resuscitative measures to the patient. It can also be helpful for physicians to explain that if a patient and/or substitute decision-maker request that resuscitative measures not be provided, the patient will still receive medically appropriate care (e.g., a patient may still be offered a surgery that is clinically indicated).
Patient Death
What can I do for my patients who are receiving end-of-life care and who wish to stay at home as long as possible or die at home?
To help patients and their caregivers (including substitute decision-makers) assess whether home care and/or dying at home are manageable options, at minimum, it is important to speak to them about the following issues:
- patient safety considerations;
- the caregiver’s ability to manage the situation; and
- whether the patient will be able to receive the necessary care (e.g., whether 24-hour, on-call coverage is required and available, whether home palliative care physicians or community-based programs are able to assist).
It is also helpful to speak with patients and their caregivers about what to expect and do, including who to contact, when the patient is about to die or has just died at home.
If a patient has expressed a wish not to be resuscitated, physicians are advised to order and complete the “Ministry of Health and Long-Term Care Do Not Resuscitate Confirmation Form” and inform the substitute decision-maker and any other caregivers about the importance of keeping the form accessible and showing it to paramedics if they are called. Unless this form is completed and presented, a paramedic is required to use resuscitative measures and transfer the patient to hospital.
When do I have to certify a patient’s death?
The Vital Statistics Act requires physicians (and in limited circumstances, nurse practitioners) who have been in attendance during or have sufficient knowledge of the last illness of a deceased person to complete and sign a medical certificate of death immediately following the death (usually interpreted as within 24 hours following death), unless there is reason to notify the coroner. Physicians cannot delegate this responsibility to others (e.g., Physician Assistants).
Completing a medical certificate of death requires planning, and so it is beneficial for physicians to designate the physician(s) or nurse practitioner(s) who will be available to attend to the deceased in order to complete and sign the medical certificate of death. It is also helpful for physicians to take into consideration any local or community strategies that are in place to facilitate the certification of death. A body can be moved to a funeral home before death is certified.
It should be noted that there is a difference between pronouncing death and certifying death. There is no legal requirement that death be pronounced by a physician, and another person, such as a nurse who was caring for the deceased, can pronounce a patient’s death. If death occurs in a hospital or long-term care home, there may be specific policies and procedures on who may pronounce death in the facility.
How do I obtain medical certificates of death?
Physicians can order blank hard copies of the medical certificate of death via phone (807-343-7432), fax (807-343-7694), or mail from the Office of the Registrar General, depending on their preference. In certain circumstances, physicians may now complete, certify, and submit medical certificates of death electronically. Physicians can access the medical certificate of death form from the Government of Ontario's Central Forms Repository: Medical Certificate of Death - Form 16.
For more guidance on how to complete medical certificates of death, see the Ontario government’s Handbook on Medical Certification of Death & Stillbirth.
Endnotes
-
Wawrzyniak v. Livingstone, 2019 ONSC 4900.
-
These forms can be ordered by completing and submitting the Government of Ontario’s “Forms Order Request.” More information about the “Ministry of Health and Long-Term Care Do Not Resuscitate Confirmation Form” is available on their website.
-
Section 35(2) of the R.R.O. 1990, Reg. 1094, General, enacted under the Vital Statistics Act, 1990; R.S.O. 1990, c. V.4. The certificate must state the cause of death according to the International Statistical Classification of Diseases and Related Health Problems, as published by the World Health Organization, and be delivered to the funeral director.
-
This may be extended on weekends, holidays and under unusual or special circumstances.
-
Section 10 of the Coroners Act, R.S.O. 1990, c. C.37 requires physicians to immediately notify a coroner or police officer if there is reason to believe that an individual has died: as a result of violence, misadventure, negligence, misconduct or malpractice; by unfair means; during pregnancy or following pregnancy in circumstances that might be reasonably attributed to the pregnancy; suddenly and unexpectedly; from disease or sickness for which they were not treated by a legally qualified medical practitioner; from any cause other than disease; or under circumstances that may require investigation.
-
Many communities in Ontario have an Expected Death in The Home Protocol.
